
Svetlana Pervykh MD1
1 DocMed Clinic of Evidence-Based Medicine, Moscow, Russia
2 Federal State Budget-Funded
Educational Institution of Higher Education “Izhevsk State Medical Academy” of the Ministry of Health of Russia (FGBOU VO IGMA of the MoH of Russia), Izhevsk, Russia
Correspondence
Svetlana Pervykh, DocMed Clinic of Evidence-Based Medicine, Trubnaya Str., 35, 108803 Moscow, Russia. Email: pervykh_s@rambler.ru
Funding information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors
Abstract
Background: Gynoid lipodystrophy is one of the most common cosmetical problems in women.
Aims: The study aims to examine the pathomorphology and histology of subcutaneous tissue in women with gynoid lipodystrophy exposed to local compression/vibration therapy using a non-invasive Beautylizer Therapy Cosmospheres V medical device.
Methods: The study enrolled 25 virtually healthy women aged 25–45 years with gynoid lipodystrophy grades I and II. The women included in the study completed a
10-session month-long therapeutic course with a non-invasive Beautylizer Therapy Cosmospheres V medical device. Bioptic punch-size samples were taken from the gluteal region prior to and following the 10-session
therapy course with the device.
Results: After completing a 10-session treatment course, a decrease in the mean adipocyte area from 123.08 ± 13.60 μm to 67.14 ± 4.20 μm was observed in punch bioptic samples of subcutaneous fat tissues of women with gynoid lipodystrophy as compared with the pre-treatment indices.
Conclusion: Thus, local application of 10-session therapy with a non-invasive Beautylizer Therapy Cosmospheres V medical device in women with gynoid lipodystrophy demonstrated a positive effect on the histological structure of the hypodermis.
K E Y W O R D S
controlled vibration, gynoid lipodystrophy, histological changes, hypodermis, vibration-compression method
1 | INTRODUC TION
Gynoid lipodystrophy (GLD) is one of the most common cosmetic problems, which, according to various data, affects 85%-98% of women aged over 20 years.1,2 The term is used to describe alter¬ations in the topography of the skin. The appeareance resemples a dimpled skin surface or an orange-peel.3 The most common location of such skin changes is the posteriors and outer side of the thighs.4,5
Gynoid lipodystrophy has a multifactorial origin.6,7 Scientists name intrinsic factors among the primary triggers of GLD occur¬rence. These are genetic predisposition, female gender, and race. For instance, European women suffer from GLD more often than Asians and representatives of the Negro race.8,9 Skin deterioration in GLD patients is caused by chronic intoxication, dietary habits (excessive consumption of fats, salt, and fast carbohydrates, leading to insu¬lin resistance), sedentary lifestyle, frequent stress, chronic somatic pathology, and hormonal imbalance.1,10,11 In particular, the problem is compounded under conditions with high levels of estrogen in the blood, such as pregnancy, breastfeeding, and long-term use of oral contraceptives.4,6,12
The main pathogenetic mechanisms of GLD include 1) hyper¬trophy of subcutaneous tissue due to an imbalance in a lipogenesis- lipolysis system with the predominance of lipogenesis, which leads to the accumulation of fat in fat cells (adipocytes)2,6,13; 2) microcircu- latory disorders, such as lymphatic and venous stasis, which lead to increased permeability of the vascular wall with the release of plasma into the interstitial space and occurrence of interstitial tissue edema, hypoxia, and endothelial damages)1,4,13; 3) conjunctive tissue densi- fication due to fibroblast activation, which leads to intensive polym-erization of derma glycosaminoglycans, elevated interstitial pressure, edema enhancement and hypoxia, and facilitates the switch of aero¬bic glycolysis to anaerobic one accompanied by lactic acid production. The excess of lactic acid activates enzymes and substances, initiating qualitative and quantitative transformation of collagen fibers, and fi- brosclerosis in interlobular conjunctive tissue septa with the forma¬tion of micronodules that are visible on the skin surface.3,4,14
Numerous methods of GLD correction are available nowa- days.6 They include physical methods, such as ultrasound, pres- sotherapy, electrostimulation, electrolipolysis, electrophoresis, vibrotherapy, vacuum therapy, endermotherapy, and infrared ir- radiation.15-17 Drug therapy (systemic enzyme therapy, injection techniques),18 external therapy (professional cosmetics for exter¬nal application, wraps),19 and invasive surgical treatment20 are also widely used for GLD treatment. However, despite the variety of available techniques, the chances of success are very limited. In addi¬tion, current GLD treatment techniques give short-term effects.4,9,15 Furthermore, there are no clear protocols for how to regulate the use and combination of different methods, and more in-depth studies are required to investigate the main processes triggered with specific methods. This study aimed to examine pathomorphological and his¬tological changes in subcutaneous tissues in women with GLD follow¬ing a combined compression-vibration treatment with a non-invasive Beautylizer Therapy Cosmoshperes V medical massage device.
2 | MATERIAL AND METHODS
The study involved 25 apparently healthy women aged 25-45 years (average age 36.71 ± 5.14 years) with grade-I and grade-II GLD symptoms. All participants underwent a combined course with com-pression and vibration using a non-invasive Beautylizer Therapy Cosmoshperes V medical massage device. The observation took 1 month to complete.
Inclusion criteria were patients aged 20-45 years, with grade-I and grade-II GLD, body mass index of 18.50-24.99 kg/m2, who signed voluntary informed consent to participate in the study. Exclusion criteria were as follows: acute or chronic somatic dis¬orders (in the acute stage, sub/decompensation phase); acute or chronic neurological disorders; infection; immunodeficiency; mental illness; cancer; skin lesions; propensity for keloid formation; tattoos in the affected zone; pregnancy; lactation; drug or alcohol abuse; any other cosmetic or therapeutic procedures <6 months before the inclusion in the study; intake of antithrombotic drugs (except for those containing acetylsalicylic acid dose of up to 100 mg/day and clopidogrel in a dose of up to 75 mg per day), as well as immunomod¬ulators, immunosuppressors, immunoglobulins, topical or systemic glucocorticoids, antihistamines, retinoids, vitamin E, and nonsteroi¬dal anti-inflammatory drugs <3 months before being included in the study. The same applies for woman participating in other clinical tri¬als (<30 days prior to study).
All women underwent a thorough screening to exclude the pres-ence of concomitant pathology or exacerbation of existing chronic pathology. Observations included clarification of complaints, history of life and disease, physical and gynecological examination, as well as laboratory (general blood and urine tests, coprogram stool test, and blood biochemistry) and instrumental testing (electrocardiogra¬phy, chest X-ray, abdominal and renal ultrasound, if necessary).
In females with GLD included in the study, local therapy with a combination of compression and vibration was applied with a non-i nvasive Beautylizer Therapy Cosmoshperes V medical device (“Economic Electrical Solutions,” Moscow). The device is a high-tech medical apparatus that performs a mechanical action on the skin using spheres of vibration. The therapy course implied 10 sessions for 1 h with a 3-day interval between sessions. The treatment regime was set automatically. At the same time, women followed their reg¬ular lifestyle and their typical diet.
Pathomorphological and histological changes in the subcutaneous fat tissue of women with GLD exposed to a combined compression-vibration treatment were studied using a bioptic punch-size sample from the gluteal fold (in the exposure area) before and after the 10-session treatment course. Biopsy sampling was carried out using a sterile disposable soft tissue biopsy needle STERYLAB (Medical Device Registration Certificate dated December 19, 2017, No. RZN 2017/5967). The biopsy material obtained was further subjected to 22-24-h fixation in a 10% solution of neutral buffered formalin, fol¬lowed by dehydration in alcohol baths with ascending concentration, soaking in xylene, and paraffin embedding. Afterward, 5-6 pm thick ultrafine sections were cut from paraffin blocks with tissue samples on the sledge microtome. The finished sections were treated with xylene to remove paraffin wax.
Tissue preparations obtained after implanted material exposure were studied after scanning glasses using a Leica Apero AT2 scan¬ner and randomly selected slices and four random FOVs. Further, the samples were dehydrated in alcohol baths of descending con-centration and stained with Mayer hematoxylin and eosin. This was followed by repeated dehydration in alcohol baths of ascending con-centration and the placement of sections in the storage environment as a permanent preparation. The results were processed and pre-sented in the Digital Pathology electronic platform.
Pathomorphological and histological changes of subcutaneous fat tissues in the bioptic punch-size sample were evaluated as per the following parameters:
Post-treatment results were compared with punch biopsy results prior to treatment initiation.
The data were statistically processed using Student’s t-test using SPSS 13.0 software package and Microsoft Excel 2013 (Microsoft, USA). The data were presented as mean (M) ± and standard devi-ations (SD). Samples were checked for normality according to the Shapiro-Wilk method. Differences were considered statistically sig-nificant at a p-value of <0.05.
2.1 | Compliance with ethical standards
The study design, its objectives and tasks, the study protocol, pa¬tient information sheet, informed consent form, confidentiality clause, and other aspects were approved by the Ethics Committee of Federal State Budget-Funded Educational Institution of Higher Education “Izhevsk State Medical Academy” of the Ministry of Health of Russia on December 22, 2020.
3 | RESULTS
The study found that non-invasive combined compression-vibration therapy with the Beautylizer Therapy Cosmoshperes V device posi-tively affects the subcutaneous fat tissue morphology in women with GLD. A significant decrease (1.83 times, p < 0.05) in average adipocyte size was observed after 10 treatment sessions from the baseline (123.08 ± 13.60 vs. 67.14 ± 4.20 pm, Figure 1, Table 1). At the same time, the average number of adipocytes in the functional fraction of adipose tissue did not change (p > 0.05) and amounted to 16.00 ± 2.00 cells.
Studying the effect of Beautylizer Therapy on the stromal component of subcutaneous tissues in women with GLD also revealed its positive effect on the exposed area. In particular, after a 10-session course of treatment with Beautylizer Therapy Cosmospheres V, a 33.4% increase from baseline in the length of interlobular septa was observed in the bioptic punch-size sample of subcutaneous fat tissues (p < 0.05). In addition, the ratio of strictly oriented/chaotically organized fibers in the interlobular stromal septa changed toward a pronounced prevalence of the former (Figure 2, Table 1).
When assessing microvessels, it was found that Beautylizer Therapy activates microcirculation in the exposure area. Thus, the vascular component per unit area of exposure zone density was sig-nificantly increased (by 32.5%, p < 0.05) in the bioptic punch-size sample of subcutaneous fat tissue in the exposed area compared with pre-t reatment values. The lumen of arterioles increased by 23.1% (p < 0.05) and the lumen of venules by 27.8% (p < 0.05) com¬pared with pre-treatment values (Figure 3).

FIGURE 1
Types of conjunctive tissue in punch bioptic samples of subcutaneous fat tissue in women with GLD after Beautylizer Therapy sessions: fat lobules (1) with adipocytes (2), stromal trabeculae (3) with strictly oriented fascicles (4). Hematoxylin and eosin staining. Microscope magnification ×1000
4 | DISCUSSION
This study examines the effect of combined therapy using com¬pression and vibration with a non-i nvasive Beautylizer Therapy Cosmoshperes V medical device on the morphological features of subcutaneous tissues of women with GLD grades I and II. The effectiveness of suggested treatment is supported by his¬tological changes in the cellular and stromal components of the hypodermis. Besides, the positive influence of Beautylizer Therapy is evidenced by a significant (p < 0.05) decrease in the average size of adipocytes compared with that before treatment after 10 sessions of the applied therapy. However, no reliable change was observed in the average number of adipocytes in the functional fraction, and no evidence of mitotic activity was ob¬tained. This could mean that the combination of compression and vibration has no or minor effect on the cell cycle. This effect on adipocyte size is likely associated with a decrease in free fatty acids entering fat cells through active transport and diffusion mechanisms.4,7,21
| Variable | Before treatment (n=25) | After treatment (n=25) |
|---|---|---|
| Average size of adipocytes, |rm | 123.08 ± 13.60 | 67.14 ± 4.20* |
| Average number of adipocytes in the functional fraction | 16.00 ± 2.00 | 16.00 ± 2.00 |
| Lumen diameter of arterioles, |rm | 14.30 ± 0.26 | 17.60 ± 0.30* |
| Lumen diameter of venules, |rm | 1.80 ± 0.41 | 2.30 ± 0.28* |
| Vascular component density per unit area of exposure zone (number of vessel lumen in FOV relative to matrix space) | 4.40 ± 0.27 | 5.83 ± 0.20* |
| Length of interlobular septa, |rm | 42.90 ± 0.15 | 57.20 ± 0.16* |
| Strictly vs. chaotically oriented fibers in stromal interlobular septa | 0.67 ± 0.024 | 0.85 ± 0.03* |
TABLE 1
Pathomorphological and histological changes in subcutaneous tissues of women suffering from GLD before and after combined exposure to local compression-vibration therapy, M ± SD
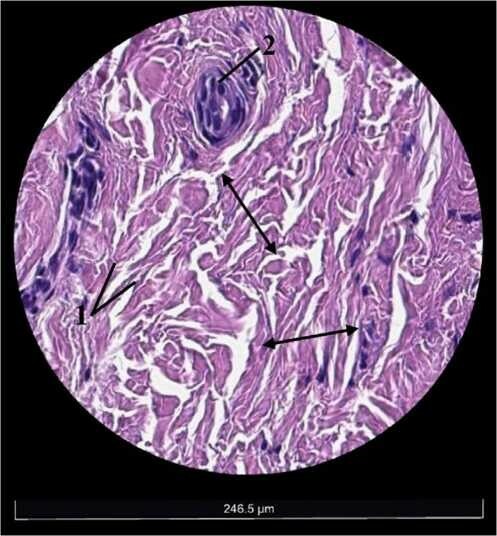
FIGURE 2
Conjunctive tissue of stromal trabeculae in the bioptic punch-size sample of subcutaneous tissue in women with GLD. Marked orientation of fibrous structures of extracellular matrix (1), visible vascular tree (2). Arrows indicate places of counting the length of groups with oriented fibers. Hematoxylin and eosin staining. Microscope magnification x1000
FIGURE 3
Microcirculatory bloodstream in punch bioptic samples of subcutaneous tissue in women with GLD after treatment sessions: blood capillaries (1), strictly oriented fiber bundles (2) in stromal trabeculae, a large number of active fibroblasts (3). Arrows indicate lengths of the vessel lumen. Hematoxylin and eosin staining. Microscope magnification x1000
The treatment with Beautylizer Therapy Cosmoshperes V had a pronounced positive effect on the stromal component of subcutane¬ous tissue, causing a substantial increase in the length of interlobular septa (by 33.4%, p < 0.05) and the number of strictly oriented vs. cha-otically organized fibers (p < 0.05) in the bioptic punch-size sample. Such an effect can be attributed to a regular external mechanical in-fluence exerted by a non-invasive Beautylizer Therapy Cosmoshperes V device (a combination of compression and vibration), facilitating changes in the orientation and distribution of collagen fibers. The applied therapy induces mechanotransduction processes, that is, the response of fibroblasts to tension, tissue geometry changes, and its spatial position. External mechanical and geometric signals play a crucial role in numerous physiological processes occurring in tissues by defining and supporting functional and structural units of tissue differentiation. Such external mechanical stimulation provokes cor¬responding biological reactions in skin tissues, namely an increase in collagen production and the formation of its strictly oriented bun¬dles in the area of trabeculae, as was observed in the patients in this study.22 It is also known that periodic mechanical stimulation of the skin increases dermal proteins and dermo-epidermal connections. This fact may indicate that it is the type of mechanical force (com¬pression, shear, and deformation) rather than its intensity that is im¬portant for the remodeling of the extracellular matrix. Besides, the extracellular matrix architectonics also directly influences the activ¬ity and functioning of the fibroblast as the main producing element of the conjunctive tissue. The change of fiber orientation influences the functional properties of skin and performs a regulatory function.22-24
One of the most important positive effects of the suggested therapy is an activation of microcirculation, which is confirmed by a statistically significant (p < 0.05) increase in the density of the vas¬cular component and vascular lumen in the exposed areas compared with corresponding indicators before treatment. This effect is signif¬icant because microcirculation disorders in subcutaneous tissues are among the leading pathogenetic mechanisms of GLD. Thus, when microcirculation is disturbed, tissue hypoxia and venous hyperoxia might occur, accompanied by decreased oxygen consumption, aer¬obic performance, and accumulation of lactic and pyruvic acids. Ultimately, all these processes cause a shift in the balance between lipolysis and lipogenesis to favor lipogenesis.2,11,25 In addition, the GLD zone is characterized by elevated pressure in capillaries and a slowdown in plasma flow due to compression and contraction of blood vessels. It may lead to an increase in capillary permeability with subsequent dermal edema, formation of thickened interlobu¬lar septa in subcutaneous fat tissue, and septa between adipocytes. Consequently, the adipocyte loses connection with the microcircula- tory channel, and fat becomes “sealed” in the cells, leading to adipo-cyte hypertrophy even in people without excess body weight.2,4,26
Applying a non-invasive Beautylizer Therapy Cosmoshperes V medical device on the skin of women with GLD intensifies microcir-culation in the exponential zone, activates lipolysis, and reduces tis¬sue hypoxia manifestations.27-30 The efficacy of various mechanical influences in GLD, in particular, compression and vibration, is proved by numerous studies. However, they address the effectiveness of ap-plying compression and vibration alone or in combination with other techniques, rather than the combination of compression and vibra¬tion, as in this study. For example, Kaminer et al.31 have shown the efficacy and safety of using a vacuum tissue disinfection device in women with moderate to severe GLD. There has been no reduction in efficiency after 1 year of use. Positive effects of vibrational ther¬apy on the skin in women with GLD were reported in a pilot study by Pilch et al.32 The study by Canela et al.17 showed that the local ap¬plication of vibration, ultrasound, and electrical stimulation reduces the thickness of the mammary fat on the sternum and increases the thickness of the skin and the contours of the contours the body. The possibilities of using and the positive effect of vibratory massage systems on the appearance of the strings in women with GLD were also presented in the study results by Adatto et al.33 and Sadowski et al.34 The study by Chieregato et al. demonstrated the advan¬tages of oscillatory vibrotherapy on body contours and skin tight¬ness.35 The study by Maia et al.36 showed a positive local effect of shock wave therapy in reducing the thickness of the fatty layer and the number of cellulite septa in the posteriors of women with GLD.
4.1 | STUDY LIMITATIONS
This study is a pilot, single-center, blinded, prospective study con-ducted on a small sample of patients with GLD grades I and II. A similar study is
4.2 | PROSPECTS FOR FURTHER RESEARCH
Studying the pathomorphological and histological changes in the subcutaneous fat tissue in women with gynoid lipodystrophy ex¬posed to local combined compression and vibration therapy on a larger sample of patients and analyzing long-term results of the ap¬plied therapy.
5 | CONCLUSIONS
A 10-s ession cource of local compression-vibration therapy with a non-invasive Beautylizer Therapy Cosmospheres V has a posi¬tive effect on the histological structure of hypodermis in women with GLD. It helped to reduce the average area of adipocytes (from 123.08 ± 13.60 to 67.14 ± 4.20 цш, p < 0.05). Other positive ef¬fects include an increase in the interlobular septa length (by 33.4%, p < 0.05) and the number of strictly oriented fibers in interlobular stromal septa. The combined therapy was found to activate the mi- crocirculatory channel, promoting an increase in the density of the vascular component (32.5%, p < 0.05) and the lumen of arterioles (23.1%, p < 0.05) and venules (27.8%, p < 0.05). Thus, the use of Beautylizer Therapy Cosmospheres allows for a significant improve¬ment of the skin structure morphology in GLD cases through avoid¬ing the use of invasive techniques.
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
ETHICAL APPROVAL
The study “Effect of combined compression-vibration therapy using non-i nvasive Beautylizer Therapy Cosmospheres V on the subcuta-neous tissue morphology in women with gynoid lipodystrophy (pilot study)” was conducted by Svetlana Pervykh and Natalya Bychkova in accordance with the ethical principles approved by the Human Experiments Ethics Committee of Federal State Budget-F unded Educational Institution of Higher Education “Izhevsk State Medical Academy” of the Ministry of Health of Russia (Protocol No. 95 of 15.02.2020). All procedures performed in studies involving human participants were in accordance with the ethical standards of the insti-tutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
DATA AVAILABILITY STATEMENT
The data are available on request.
REFERENCES














Filiaalid: USA
Astralumis LLC
7201 W Palmetto Park Rd
Boca Raton Florida, FL33433
TEL: +1 768 513 4589
Riia , Läti . Pernavas 2 LV1012
info@beautylizer.eu
+371 29115005
Headqarter: Beautylizer Aesthetic Medical Equipment Trading LLC, Dubai, PO Box 21495
Filiaalid: USA
Astralumis LLC
7201 W Palmetto Park Rd
Boca Raton Florida, FL33433
TEL: +1 768 513 4589
Riia , Läti . Pernavas 2 LV1012
info@beautylizer.eu
+371 29115005
Headqarter: Beautylizer Aesthetic Medical Equipment Trading LLC, Dubai, PO Box 21495
Filiaalid: USA
Astralumis LLC
7201 W Palmetto Park Rd
Boca Raton Florida, FL33433
TEL: +1 768 513 4589
Riia , Läti . Pernavas 2 LV1012
info@beautylizer.eu
+371 29115005
Headqarter: Beautylizer Aesthetic Medical Equipment Trading LLC, Dubai, PO Box 21495